Anemia in Pregnancy – Causes, Symptoms, Investigations, Complications Treatment Explained
Below is a **complete, concise-but-exhaustive, exam-ready medical reference** for **Anemia in Pregnancy**, following the structured pattern you prefer (definition → pathophysiology → causes → clinical features → investigations → differential diagnosis → management → drug details → monitoring → counselling).
Images included for quick visual recall.
---
#

# **ANEMIA IN PREGNANCY — COMPLETE REFERENCE**
---
## **1. Definition**
* **WHO definition during pregnancy:**
* **Hb <11 g/dL** (1st & 3rd trimester)
* **Hb <10.5 g/dL** (2nd trimester)
* **Severity (India guidelines):**
* Mild: 10–10.9 g/dL
* Moderate: 7–9.9 g/dL
* Severe: 4–6.9 g/dL
* Very severe: <4 g/dL
---
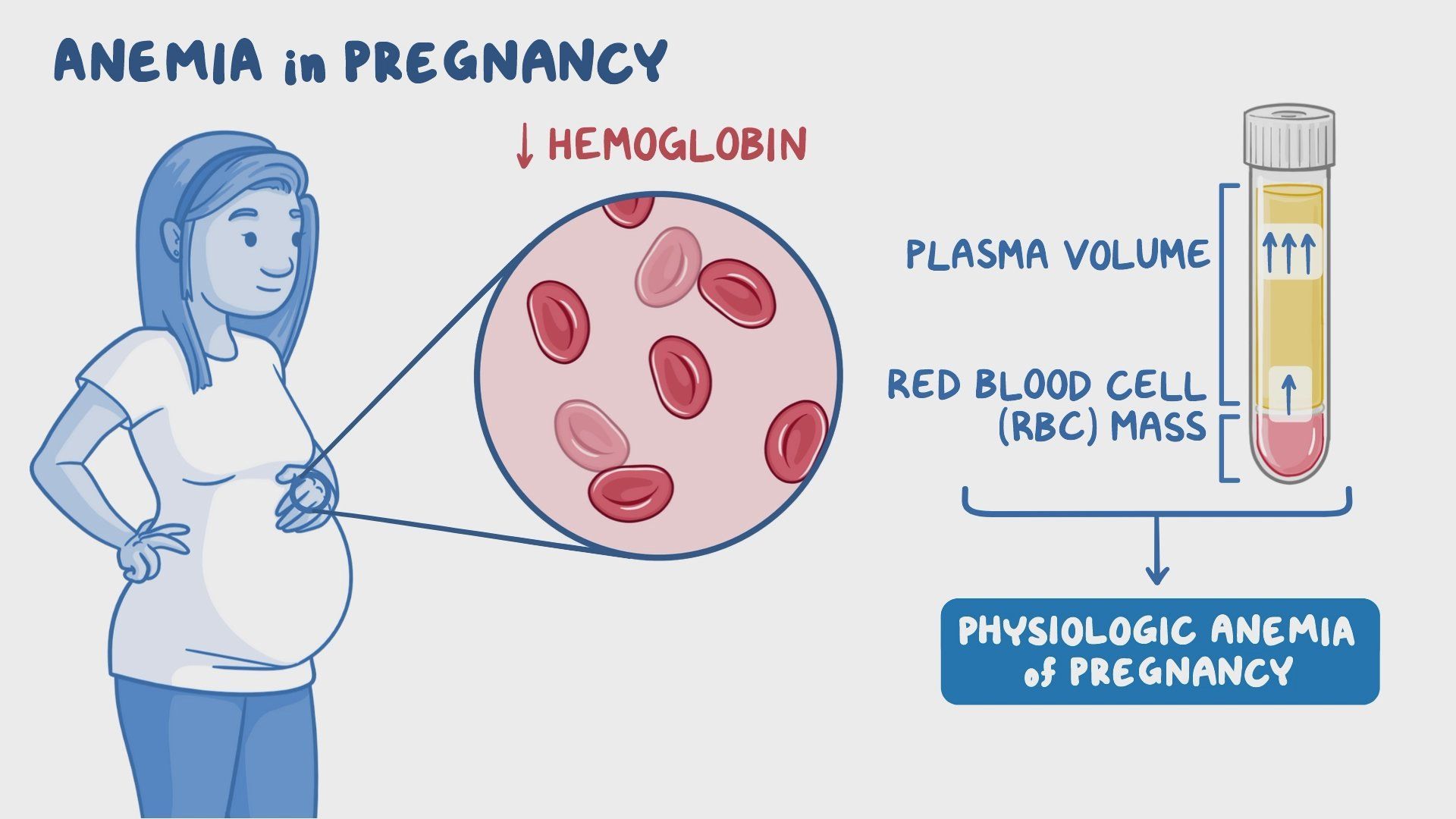
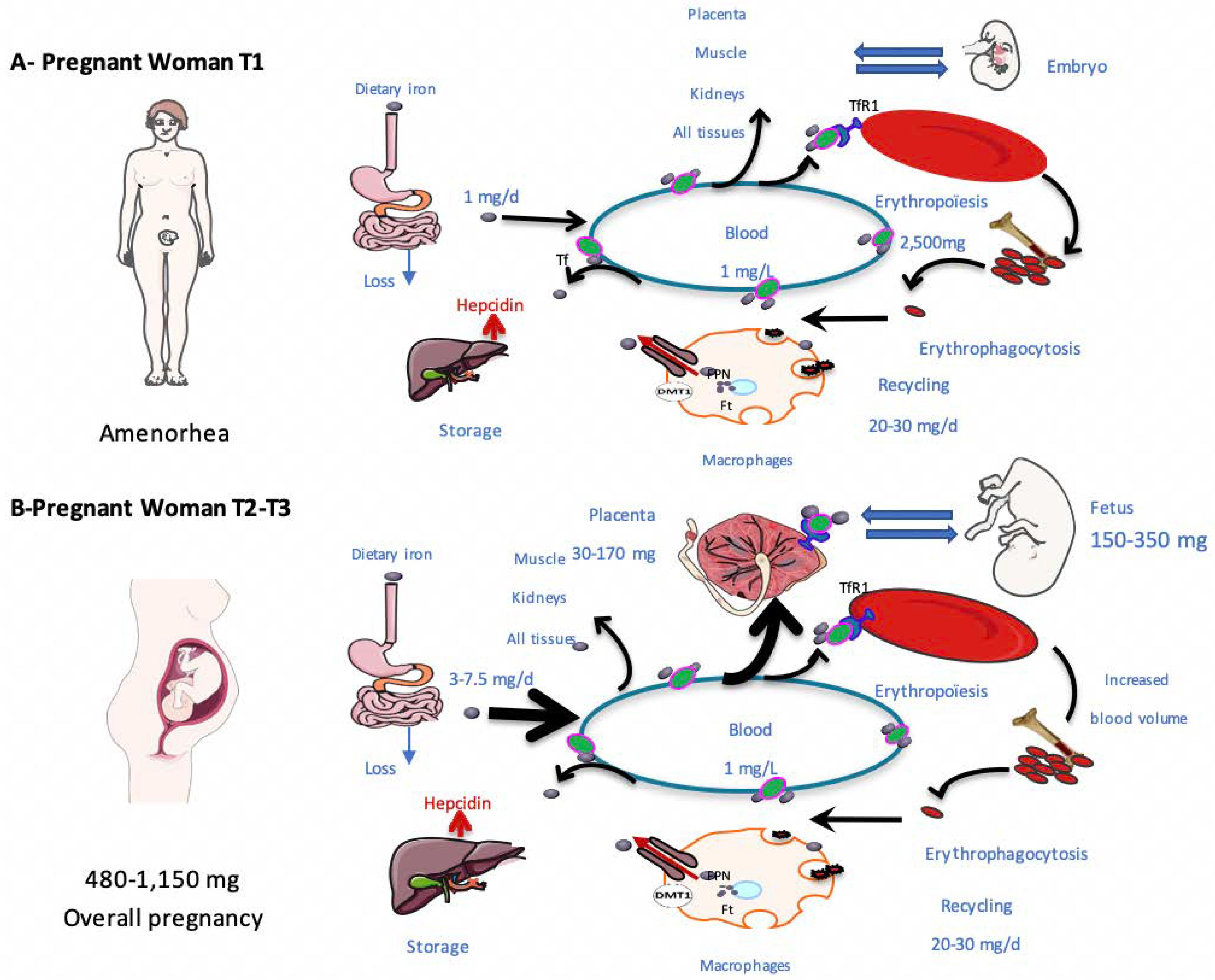
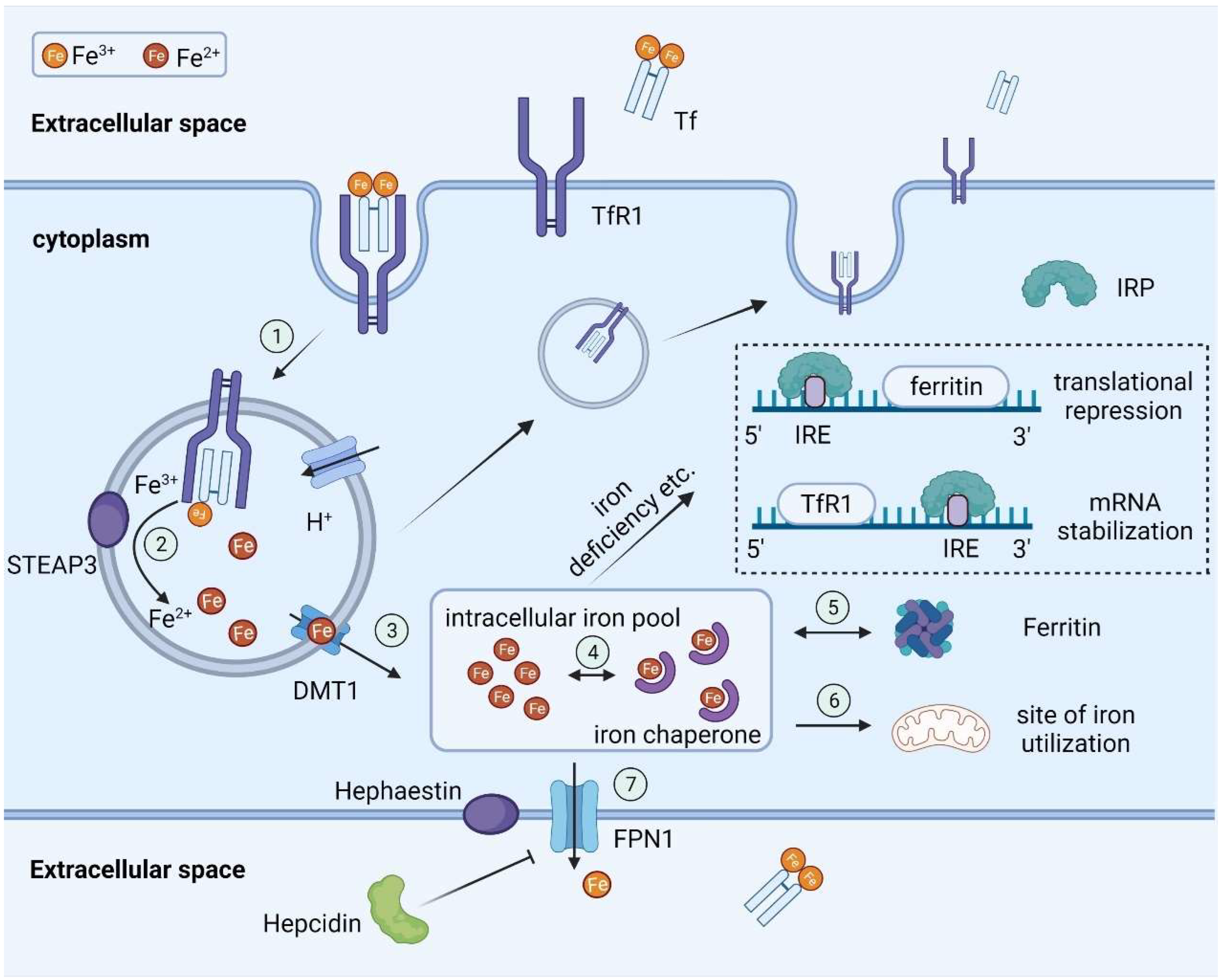
## **2. Pathophysiology**
Pregnancy causes:
* **↑ Plasma volume (40–50%) → hemodilution**
* **↑ Iron demand (1000 mg total in pregnancy)**
* 300 mg fetus + 500 mg maternal RBC mass + 200 mg losses
* **Relative deficiency** occurs if intake/absorption inadequate.
* Commonest type = **Iron Deficiency Anemia (IDA)**.
---
## **3. Causes**
### **A. Nutritional**
* Iron deficiency (most common)
* Folate deficiency
* Vitamin B12 deficiency
### **B. Hematological**
* Thalassemia trait / Thalassemia major
* Sickle cell disease
* Aplastic anemia
### **C. Secondary to disease**
* Anemia of chronic disease
* Malaria
* Hookworm
* Hemolytic anemia
---
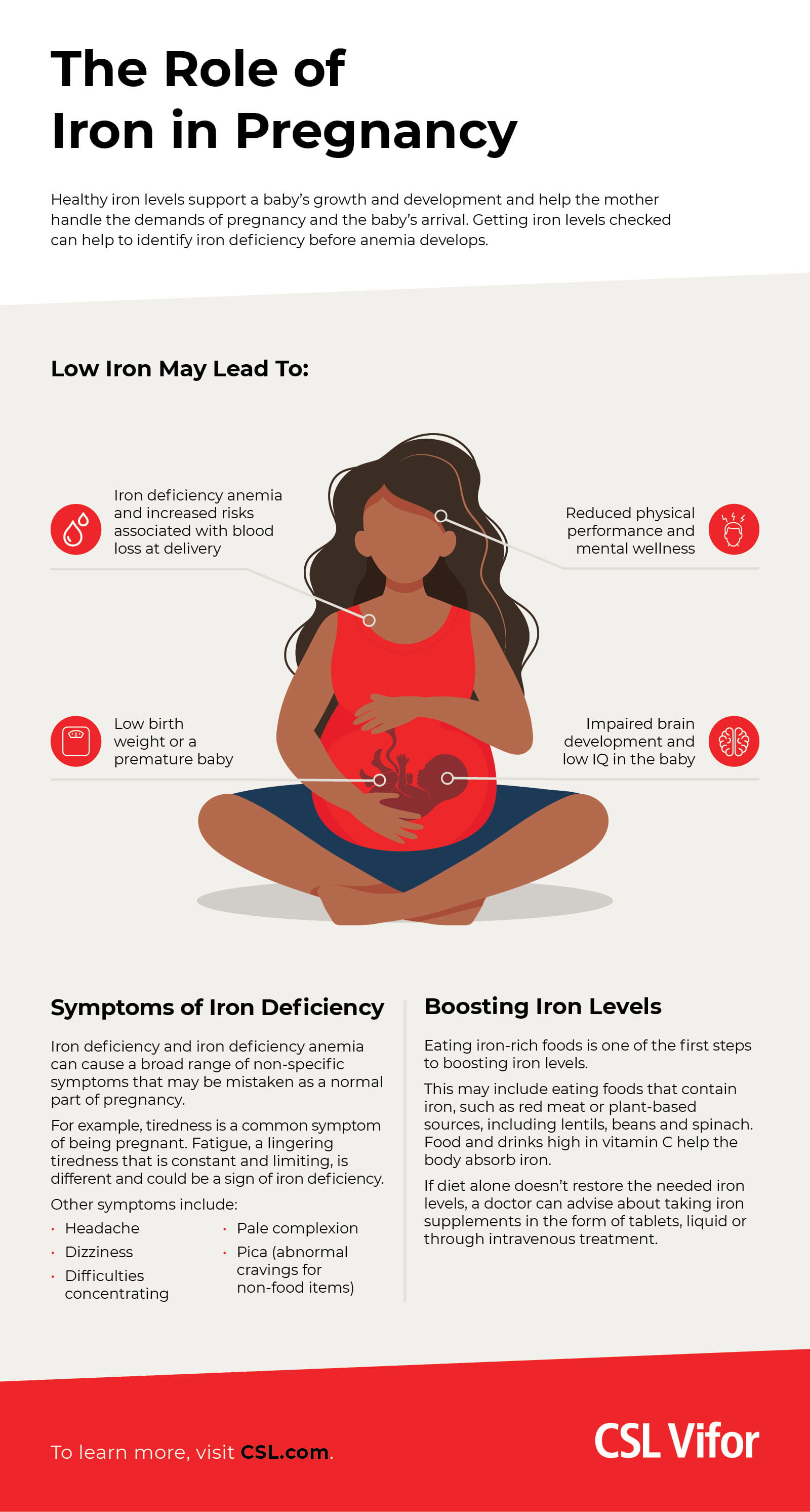
## **4. Clinical Features**
* Fatigue, weakness, palpitations, dyspnea
* Pallor: conjunctiva, tongue, nails
* Glossitis, angular stomatitis (in IDA)
* Pica
* Jaundice → suggest hemolysis
* Systolic murmur due to hyperdynamic circulation
---
## **5. Maternal Complications**
* Preterm labor
* PPH (poor uterine muscle function)
* Cardiac failure (especially Hb <5 g/dL)
* Increased infections
* Poor lactation
---
## **6. Fetal Complications**
* IUGR
* LBW
* Preterm birth
* Fetal hypoxia
* Stillbirth (severe anemia)
---
#





---
## **7. Investigations**
### **A. Basic**
1. **CBC**
* Hb, Hct (PCV), RBC indices
* **MCV <80 fL → microcytic**
* **MCHC low → hypochromia**
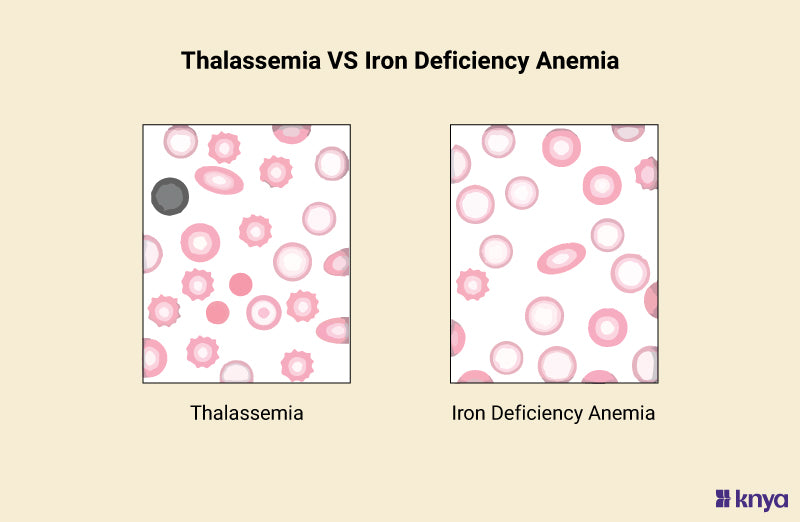
2. **Peripheral Smear**
* IDA: microcytic, hypochromic, anisopoikilocytosis
* Megaloblastic: macro-ovalocytes, hypersegmented neutrophils
3. **Reticulocyte count**
* Low → production problem
* High → hemolysis / blood loss
### **B. Iron Studies**
| Parameter | Iron Deficiency | Anemia of Chronic disease |
| ---------------------- | --------------- | ------------------------- |
| Serum Iron | ↓ | ↓ |
| TIBC | ↑ | ↓ / normal |
| Ferritin | ↓ | ↑ |
| Transferrin saturation | ↓ | ↓ |
### **C. RBC Indices**
* **Mentzer Index = MCV / RBC count**
* > 13 → IDA
* <13 → Thalassemia trait
### **D. Others**
* Hb Electrophoresis → thalassemia/sickle
* Stool exam → worms
* LFT/RFT if severe
---
## **8. Differential Diagnosis**
* Iron Deficiency Anemia
* Thalassemia trait
* Anemia of chronic disease
* Sickle cell disease
* Megaloblastic anemia
* Hemolytic anemia
---
# **9. Management (Stepwise)**
## **Step 1: Confirm type of anemia (CBC + smear + ferritin)**
* If ferritin <30 ng/mL → IDA
* If normal ferritin + low MCV → thalassemia trait
* If macrocytic → folate/B12 deficiency
---
## **Step 2: Treatment Based on Severity**
### **A. Mild to Moderate IDA (Hb 7–10.9 g/dL)**
**Oral Iron Therapy**
* **Elemental iron 100–200 mg/day**
* Examples: Ferrous sulfate 325 mg = 65 mg elemental
* Take on empty stomach ± vitamin C
* Avoid with tea/coffee/milk (↓ absorption)
### **B. Severe Anemia (Hb <7 g/dL)**
* **IV Iron** OR **Blood transfusion** (if near-term, cardiac failure, or Hb <5 g/dL)
### **C. Megaloblastic Anemia**
* **Folic acid 5 mg/day**
* **Vitamin B12: 1000 µg IM weekly × 4 → monthly**
### **D. Thalassemia trait**
* Avoid excess iron
* Genetic counselling
---
## **10. IV Iron Therapy (Detailed)**
### **Indications**
* Intolerance to oral iron
* Malabsorption
* Hb <7 g/dL and stable
* Late pregnancy and need rapid correction
### **Common IV Preparations**
#### **1. Iron Sucrose**
* Dose: 200 mg IV per sitting
* Give multiple sittings until total requirement met
* AE: hypotension, nausea
* Safe in pregnancy
#### **2. Ferric Carboxymaltose (FCM)**
* Dose: Up to **1000 mg in a single sitting**
* Faster replenishment
* Less infusion reactions
### **Calculation of Total Iron Requirement**
`Total iron dose (mg) = [2.4 × (Target Hb – Actual Hb) × weight (kg)] + 500 mg (stores)`
---
## **11. Blood Transfusion**
**Indications**
* Hb <5 g/dL (any trimester)
* Hb <7 g/dL + labor / imminent surgery
* Cardiac failure
* Severe symptoms with hypoxia
---
# **12. Non-Pharmacologic Measures**
* Iron-rich diet: green leafy vegetables, jaggery, legumes, red meat
* Deworming (Albendazole 400 mg once after 2nd trimester)
* Treat malaria
* Birth spacing
* Cooking in iron utensils
---
# **13. Drug Details (As Required by Your Pattern)**
---
## **A. ORAL IRON**
### **Indication:** IDA
### **MOA:** Converted to ferrous form → absorbed in duodenum → used for Hb synthesis
### **Dose:** 100–200 mg elemental iron/day
### **PK:** Absorbed in proximal small intestine; excreted minimally
### **Common AE:** Nausea, constipation, black stools
### **Serious AE:** Very rare GI bleeding
### **Contraindications:** Hemochromatosis, hemolytic anemia
### **Drug interactions:** Antacids, tetracyclines, tea/coffee reduce absorption
### **Monitoring:** Hb every 4 weeks
### **Counselling:** Take on empty stomach; Vitamin C improves absorption
---
## **B. FOLIC ACID**
### **Indication:** Megaloblastic anemia, prevention of NTD
### **MOA:** DNA/RNA synthesis
### **Dose:** 5 mg/day for anemia; 400 µg/day for prophylaxis
### **AE:** Rare rash
### **Interactions:** Anticonvulsants reduce folate levels
### **Monitoring:** Hb, MCV
---
## **C. VITAMIN B12 (CYANOCOBALAMIN)**
### **Indication:** B12 deficiency
### **MOA:** DNA synthesis + myelin formation
### **Dose:** 1000 µg IM weekly × 4 → monthly
### **AE:** Flushing, hypokalemia early
### **Contraindications:** Leber hereditary optic neuropathy
### **Monitoring:** Reticulocyte response in 1 week
---
## **D. IV IRON (FCM / Iron Sucrose)**
### **Indication:** Severe IDA; intolerance to oral iron
### **MOA:** Direct replenishment of iron stores
### **Dose:** Based on calculation
### **AE:** Hypersensitivity, hypotension
### **Monitoring:** Hb after 2–3 weeks
---
# **14. National Programs (India)**
## **I-NIAP (Intensified National Iron Plus Initiative Program)**
* Daily supplementation:
* Pregnant women: **60 mg elemental iron + 500 µg folic acid** × 180 days
* Biweekly deworming
* Screening for anemia at each ANC visit
## **Anemia Mukt Bharat — 6×6×6 Strategy**
**6 Target beneficiaries** (children, adolescents, pregnant women, etc.)
**6 Interventions**
1. Iron–folic acid supplementation
2. Deworming
3. Behavior change communication
4. Testing & treatment
5. Intensified year-round IEC
6. Parenteral iron therapy
**6 Institutional mechanisms** (logistics, training, monitoring etc.)
---
# **15. Iron Requirements During Pregnancy**
* Additional requirement ≈ **1000 mg total**
* Daily need = **4–6 mg absorbed iron/day**
* Dietary intake usually insufficient → supplementation needed
---
If you want, I can also generate:
✅ **20–30 case-based MCQs**
✅ **HTML/CSS/JS interactive quiz (exam mode)**
✅ **SEO title, description & keywords**
✅ **Infographics or generated images**
Just tell me **which output you want next**.
Images included for quick visual recall.
---
#




# **ANEMIA IN PREGNANCY — COMPLETE REFERENCE**
---
## **1. Definition**
* **WHO definition during pregnancy:**
* **Hb <11 g/dL** (1st & 3rd trimester)
* **Hb <10.5 g/dL** (2nd trimester)
* **Severity (India guidelines):**
* Mild: 10–10.9 g/dL
* Moderate: 7–9.9 g/dL
* Severe: 4–6.9 g/dL
* Very severe: <4 g/dL
---
## **2. Pathophysiology**
Pregnancy causes:
* **↑ Plasma volume (40–50%) → hemodilution**
* **↑ Iron demand (1000 mg total in pregnancy)**
* 300 mg fetus + 500 mg maternal RBC mass + 200 mg losses
* **Relative deficiency** occurs if intake/absorption inadequate.
* Commonest type = **Iron Deficiency Anemia (IDA)**.
---
## **3. Causes**
### **A. Nutritional**
* Iron deficiency (most common)
* Folate deficiency
* Vitamin B12 deficiency
### **B. Hematological**
* Thalassemia trait / Thalassemia major
* Sickle cell disease
* Aplastic anemia
### **C. Secondary to disease**
* Anemia of chronic disease
* Malaria
* Hookworm
* Hemolytic anemia
---
## **4. Clinical Features**
* Fatigue, weakness, palpitations, dyspnea
* Pallor: conjunctiva, tongue, nails
* Glossitis, angular stomatitis (in IDA)
* Pica
* Jaundice → suggest hemolysis
* Systolic murmur due to hyperdynamic circulation
---
## **5. Maternal Complications**
* Preterm labor
* PPH (poor uterine muscle function)
* Cardiac failure (especially Hb <5 g/dL)
* Increased infections
* Poor lactation
---
## **6. Fetal Complications**
* IUGR
* LBW
* Preterm birth
* Fetal hypoxia
* Stillbirth (severe anemia)
---
#








---
## **7. Investigations**
### **A. Basic**
1. **CBC**
* Hb, Hct (PCV), RBC indices
* **MCV <80 fL → microcytic**
* **MCHC low → hypochromia**
2. **Peripheral Smear**
* IDA: microcytic, hypochromic, anisopoikilocytosis
* Megaloblastic: macro-ovalocytes, hypersegmented neutrophils
3. **Reticulocyte count**
* Low → production problem
* High → hemolysis / blood loss
### **B. Iron Studies**
| Parameter | Iron Deficiency | Anemia of Chronic disease |
| ---------------------- | --------------- | ------------------------- |
| Serum Iron | ↓ | ↓ |
| TIBC | ↑ | ↓ / normal |
| Ferritin | ↓ | ↑ |
| Transferrin saturation | ↓ | ↓ |
### **C. RBC Indices**
* **Mentzer Index = MCV / RBC count**
* > 13 → IDA
* <13 → Thalassemia trait
### **D. Others**
* Hb Electrophoresis → thalassemia/sickle
* Stool exam → worms
* LFT/RFT if severe
---
## **8. Differential Diagnosis**
* Iron Deficiency Anemia
* Thalassemia trait
* Anemia of chronic disease
* Sickle cell disease
* Megaloblastic anemia
* Hemolytic anemia
---
# **9. Management (Stepwise)**
## **Step 1: Confirm type of anemia (CBC + smear + ferritin)**
* If ferritin <30 ng/mL → IDA
* If normal ferritin + low MCV → thalassemia trait
* If macrocytic → folate/B12 deficiency
---
## **Step 2: Treatment Based on Severity**
### **A. Mild to Moderate IDA (Hb 7–10.9 g/dL)**
**Oral Iron Therapy**
* **Elemental iron 100–200 mg/day**
* Examples: Ferrous sulfate 325 mg = 65 mg elemental
* Take on empty stomach ± vitamin C
* Avoid with tea/coffee/milk (↓ absorption)
### **B. Severe Anemia (Hb <7 g/dL)**
* **IV Iron** OR **Blood transfusion** (if near-term, cardiac failure, or Hb <5 g/dL)
### **C. Megaloblastic Anemia**
* **Folic acid 5 mg/day**
* **Vitamin B12: 1000 µg IM weekly × 4 → monthly**
### **D. Thalassemia trait**
* Avoid excess iron
* Genetic counselling
---
## **10. IV Iron Therapy (Detailed)**
### **Indications**
* Intolerance to oral iron
* Malabsorption
* Hb <7 g/dL and stable
* Late pregnancy and need rapid correction
### **Common IV Preparations**
#### **1. Iron Sucrose**
* Dose: 200 mg IV per sitting
* Give multiple sittings until total requirement met
* AE: hypotension, nausea
* Safe in pregnancy
#### **2. Ferric Carboxymaltose (FCM)**
* Dose: Up to **1000 mg in a single sitting**
* Faster replenishment
* Less infusion reactions
### **Calculation of Total Iron Requirement**
`Total iron dose (mg) = [2.4 × (Target Hb – Actual Hb) × weight (kg)] + 500 mg (stores)`
---
## **11. Blood Transfusion**
**Indications**
* Hb <5 g/dL (any trimester)
* Hb <7 g/dL + labor / imminent surgery
* Cardiac failure
* Severe symptoms with hypoxia
---
# **12. Non-Pharmacologic Measures**
* Iron-rich diet: green leafy vegetables, jaggery, legumes, red meat
* Deworming (Albendazole 400 mg once after 2nd trimester)
* Treat malaria
* Birth spacing
* Cooking in iron utensils
---
# **13. Drug Details (As Required by Your Pattern)**
---
## **A. ORAL IRON**
### **Indication:** IDA
### **MOA:** Converted to ferrous form → absorbed in duodenum → used for Hb synthesis
### **Dose:** 100–200 mg elemental iron/day
### **PK:** Absorbed in proximal small intestine; excreted minimally
### **Common AE:** Nausea, constipation, black stools
### **Serious AE:** Very rare GI bleeding
### **Contraindications:** Hemochromatosis, hemolytic anemia
### **Drug interactions:** Antacids, tetracyclines, tea/coffee reduce absorption
### **Monitoring:** Hb every 4 weeks
### **Counselling:** Take on empty stomach; Vitamin C improves absorption
---
## **B. FOLIC ACID**
### **Indication:** Megaloblastic anemia, prevention of NTD
### **MOA:** DNA/RNA synthesis
### **Dose:** 5 mg/day for anemia; 400 µg/day for prophylaxis
### **AE:** Rare rash
### **Interactions:** Anticonvulsants reduce folate levels
### **Monitoring:** Hb, MCV
---
## **C. VITAMIN B12 (CYANOCOBALAMIN)**
### **Indication:** B12 deficiency
### **MOA:** DNA synthesis + myelin formation
### **Dose:** 1000 µg IM weekly × 4 → monthly
### **AE:** Flushing, hypokalemia early
### **Contraindications:** Leber hereditary optic neuropathy
### **Monitoring:** Reticulocyte response in 1 week
---
## **D. IV IRON (FCM / Iron Sucrose)**
### **Indication:** Severe IDA; intolerance to oral iron
### **MOA:** Direct replenishment of iron stores
### **Dose:** Based on calculation
### **AE:** Hypersensitivity, hypotension
### **Monitoring:** Hb after 2–3 weeks
---
# **14. National Programs (India)**
## **I-NIAP (Intensified National Iron Plus Initiative Program)**
* Daily supplementation:
* Pregnant women: **60 mg elemental iron + 500 µg folic acid** × 180 days
* Biweekly deworming
* Screening for anemia at each ANC visit
## **Anemia Mukt Bharat — 6×6×6 Strategy**
**6 Target beneficiaries** (children, adolescents, pregnant women, etc.)
**6 Interventions**
1. Iron–folic acid supplementation
2. Deworming
3. Behavior change communication
4. Testing & treatment
5. Intensified year-round IEC
6. Parenteral iron therapy
**6 Institutional mechanisms** (logistics, training, monitoring etc.)
---
# **15. Iron Requirements During Pregnancy**
* Additional requirement ≈ **1000 mg total**
* Daily need = **4–6 mg absorbed iron/day**
* Dietary intake usually insufficient → supplementation needed
---
If you want, I can also generate:
✅ **20–30 case-based MCQs**
✅ **HTML/CSS/JS interactive quiz (exam mode)**
✅ **SEO title, description & keywords**
✅ **Infographics or generated images**
Just tell me **which output you want next**.




















Comments (3)

Medical Student
This was incredibly helpful for my upcoming exam. Thank you!
Nursing Professional
Great explanation of the ECG changes in hyperkalemia!