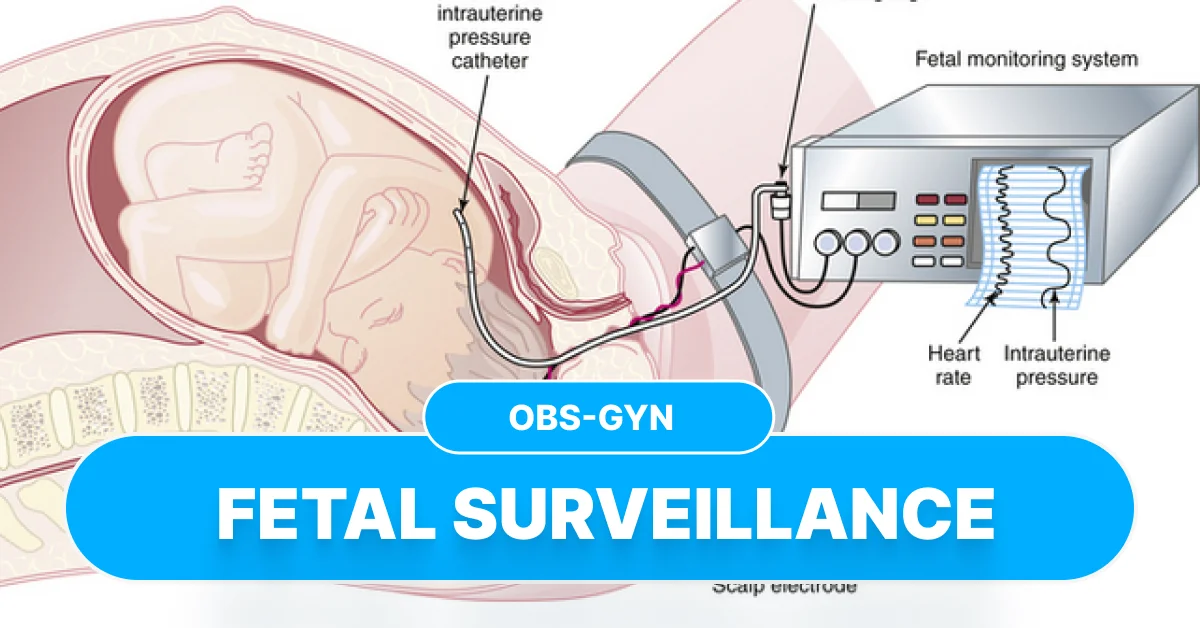
Antepartum Fetal Monitoring — Methods, Interpretation, Indications, NST, BPP Doppler Explained
Below is a **complete, concise but full-detail reference** on **Antepartum Fetal Monitoring**, perfect for notes, exams, and SEO-optimized blog posting.
---
# **Antepartum Fetal Monitoring — Complete Guide**



## **SEO Title**
**Antepartum Fetal Monitoring: Methods, Interpretation, Indications & Clinical Management**
## **SEO Description**
A complete guide to antepartum fetal monitoring including NST, CST, BPP, modified BPP, Doppler velocimetry, fetal movement counting, indications, interpretation criteria, and clinical decision-making.
## **SEO Keywords**
Antepartum fetal monitoring, NST, CST, Biophysical profile, Modified BPP, Doppler velocimetry, fetal surveillance, high-risk pregnancy monitoring, umbilical artery doppler, fetal wellbeing tests.
---
# ⭐ **1. Introduction**
Antepartum fetal monitoring refers to **non-invasive tests done during pregnancy (after viability)** to assess **fetal oxygenation, wellbeing, and risk of hypoxia/acidemia** before labor.
**Main Goals:**
* Detect early fetal compromise
* Reduce stillbirth
* Decide timing of delivery in high-risk pregnancies
---
# ⭐ **2. Physiological Basis**
Fetal well-being is reflected by:
* **Heart rate reactivity** → Indicates intact autonomic system + adequate oxygenation.
* **Fetal movements, tone, breathing** → Reflect CNS integrity.
* **Amniotic fluid volume** → Marker of long-standing placental perfusion.
* **Placental blood flow** → Assessed via Dopplers.
---
# ⭐ **3. Indications for Antepartum Fetal Surveillance**
### **Maternal Causes**
* Diabetes (GDM/Type 1/Type 2)
* Hypertensive disorders (GHTN, Pre-eclampsia)
* Cholestasis of pregnancy
* SLE, APS
* Chronic kidney disease
* Rh isoimmunization
* Post-term pregnancy
### **Fetal Causes**
* FGR (IUGR)
* Decreased fetal movements
* Oligohydramnios/polyhydramnios
* Multiple pregnancy (esp. monochorionic)
* Congenital anomalies
### **Placental Causes**
* Placental insufficiency
* Placenta previa with bleeding
---
# ⭐ **4. Methods of Antepartum Fetal Monitoring**
---
## **4.1 Fetal Movement Counting (Kick Count)**
Simple maternal awareness test.
### **Protocols**
* **Cardiff: 10 movements within 12 hours**
* **Count-to-ten: 10 kicks in ≤2 hours**
* If <4 in 1 hour → repeat → if still decreased → NST
---
## **4.2 Non-Stress Test (NST)**
Records fetal heart rate (FHR) in relation to movements.
### **Principle**
**Accelerations = Reassuring indicator of fetal oxygenation and autonomic function.**
### **Procedure**
* Duration: 20 minutes (extend to 40 min if non-reactive)
* Interpretation based on ≥32 weeks criteria.
### **NST Interpretation**
#### **Reactive NST**
* **≥2 accelerations** in 20 min
* Acceleration: **≥15 bpm for ≥15 sec** (≥10 bpm for ≥10 sec if <32 weeks)
**Significance:** Normal fetal oxygenation.
#### **Non-Reactive NST**
* <2 accelerations in 40 minutes
* Could be due to sleep cycle/hypoxia/CNS depression.
👉 **Next step:** BPP or CST.
---
## **4.3 Contraction Stress Test (CST) / Oxytocin Challenge Test**
Evaluates **FHR response to induced uterine contractions** → stresses placenta.
### **Method**
* Use nipple stimulation or dilute oxytocin.
### **Positive CST**
* **Late decelerations** with ≥50% contractions
### **Interpretation**
* **Negative CST:** No late decels → reassuring
* **Positive CST:** Repetitive late decels → **Delivery needed**
* **Equivocal:** Intermittent decels
---
## **4.4 Biophysical Profile (BPP)**
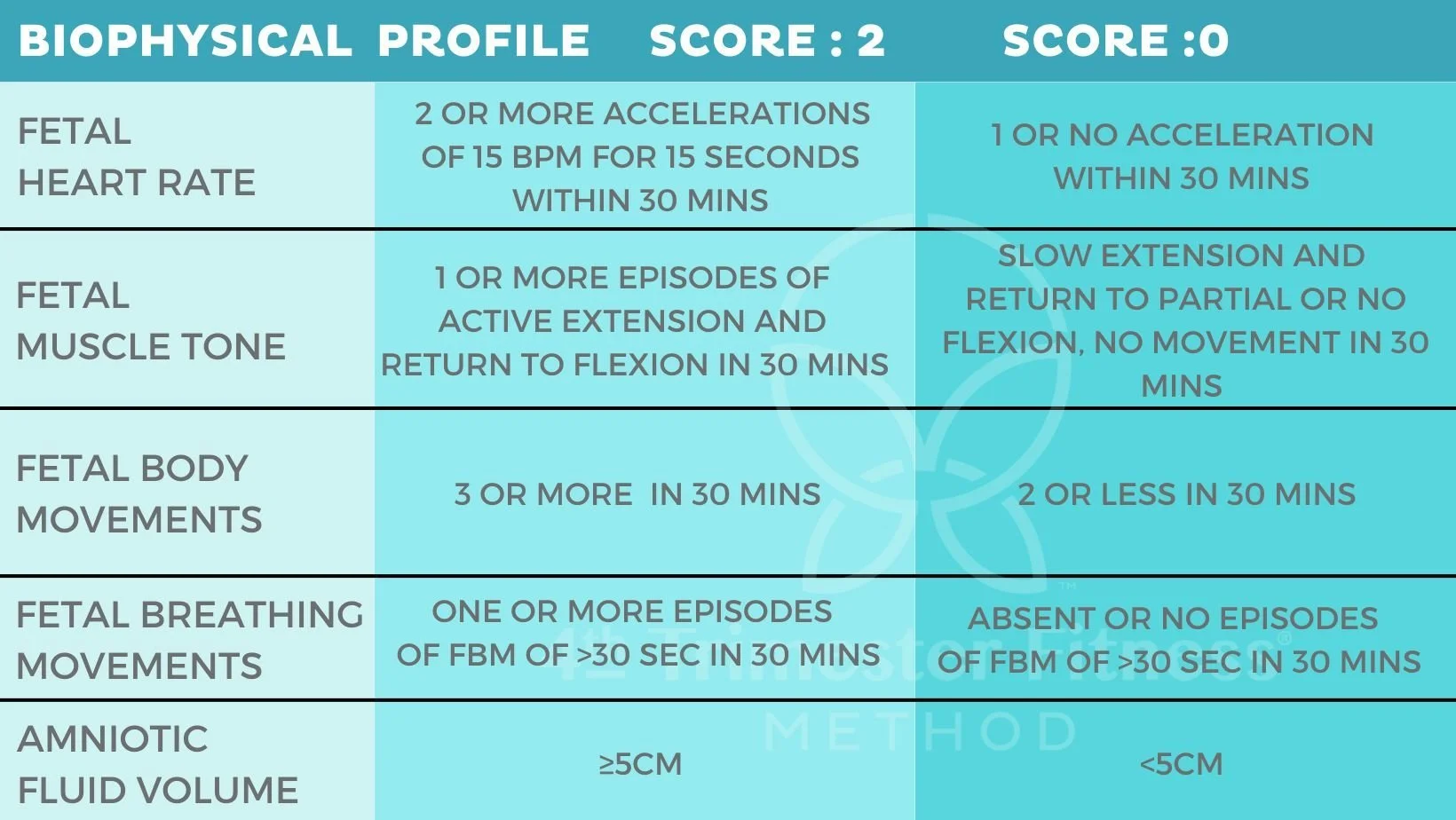

Five parameters (each scored 0 or 2):
1. **NST**
2. **Fetal breathing movements**
3. **Gross body movements**
4. **Fetal tone**
5. **Amniotic fluid volume** (Single deepest pocket ≥2 cm)
### **Scoring**
| Score | Interpretation |
| -------- | -------------------------------- |
| **8–10** | Normal |
| **6** | Equivocal — repeat in 24 hrs |
| **≤4** | Abnormal → **Consider delivery** |
---
## **4.5 Modified BPP**
* **NST + Amniotic Fluid Index (AFI)**
Normal if:
* Reactive NST **AND** AFI >5 cm
---
## **4.6 Doppler Velocimetry**
Essential in **FGR, placental insufficiency, preeclampsia**.
### **Umbilical Artery Doppler**
* **Normal:** High diastolic flow
* **Abnormal findings:**
* **Increased S/D ratio** (placental resistance)
* **Absent end-diastolic flow (AEDF)**
* **Reversed end-diastolic flow (REDF)** → **severe compromise** → urgent delivery
### **Middle Cerebral Artery (MCA) Doppler**
* Low resistance → brain sparing in hypoxia.
* Used in **anemia** (MCA PSV >1.5 MoM).
### **Ductus Venosus Doppler**
* Abnormal A-wave → impending fetal acidemia.
---
# ⭐ **5. Interpretation Summary Table**
| Test | Normal | Abnormal |
| --------------------- | ---------------------- | ---------------------- |
| **Kick Count** | 10 kicks ≤2 hrs | <4/hr or ↓ movements |
| **NST** | Reactive | Non-reactive |
| **CST** | Negative | Positive (late decels) |
| **BPP** | 8–10 | ≤4 |
| **Modified BPP** | Reactive + AFI >5 | Any abnormal |
| **Umb. Art. Doppler** | Forward diastolic flow | AEDF/REDF |
---
# ⭐ **6. Clinical Decision Making**
### If **NST reactive** → Continue routine surveillance
### If **NST non-reactive** → Do BPP or CST
### If **BPP ≤4** → **Deliver**
### If **CST positive** → **Deliver**
### If **Umbilical artery REDF** → **Immediate delivery** (after steroid coverage if possible)
---
# ⭐ **7. Frequency of Testing**
| Condition | Frequency |
| ---------------------- | ------------------ |
| Diabetes, hypertension | Weekly or biweekly |
| FGR | 2–3 times/week |
| Post-term | Daily NST/BPP |
| Oligohydramnios | 2–3 times/week |
---
If you want, I can also generate:
✅ **30 case scenarios with management**
✅ **20–30 MCQs (exam-style)**
✅ **HTML/CSS/JS interactive quiz**
✅ **Printable PDF notes**
Just tell me what you need!
---
# **Antepartum Fetal Monitoring — Complete Guide**




## **SEO Title**
**Antepartum Fetal Monitoring: Methods, Interpretation, Indications & Clinical Management**
## **SEO Description**
A complete guide to antepartum fetal monitoring including NST, CST, BPP, modified BPP, Doppler velocimetry, fetal movement counting, indications, interpretation criteria, and clinical decision-making.
## **SEO Keywords**
Antepartum fetal monitoring, NST, CST, Biophysical profile, Modified BPP, Doppler velocimetry, fetal surveillance, high-risk pregnancy monitoring, umbilical artery doppler, fetal wellbeing tests.
---
# ⭐ **1. Introduction**
Antepartum fetal monitoring refers to **non-invasive tests done during pregnancy (after viability)** to assess **fetal oxygenation, wellbeing, and risk of hypoxia/acidemia** before labor.
**Main Goals:**
* Detect early fetal compromise
* Reduce stillbirth
* Decide timing of delivery in high-risk pregnancies
---
# ⭐ **2. Physiological Basis**
Fetal well-being is reflected by:
* **Heart rate reactivity** → Indicates intact autonomic system + adequate oxygenation.
* **Fetal movements, tone, breathing** → Reflect CNS integrity.
* **Amniotic fluid volume** → Marker of long-standing placental perfusion.
* **Placental blood flow** → Assessed via Dopplers.
---
# ⭐ **3. Indications for Antepartum Fetal Surveillance**
### **Maternal Causes**
* Diabetes (GDM/Type 1/Type 2)
* Hypertensive disorders (GHTN, Pre-eclampsia)
* Cholestasis of pregnancy
* SLE, APS
* Chronic kidney disease
* Rh isoimmunization
* Post-term pregnancy
### **Fetal Causes**
* FGR (IUGR)
* Decreased fetal movements
* Oligohydramnios/polyhydramnios
* Multiple pregnancy (esp. monochorionic)
* Congenital anomalies
### **Placental Causes**
* Placental insufficiency
* Placenta previa with bleeding
---
# ⭐ **4. Methods of Antepartum Fetal Monitoring**
---
## **4.1 Fetal Movement Counting (Kick Count)**
Simple maternal awareness test.
### **Protocols**
* **Cardiff: 10 movements within 12 hours**
* **Count-to-ten: 10 kicks in ≤2 hours**
* If <4 in 1 hour → repeat → if still decreased → NST
---
## **4.2 Non-Stress Test (NST)**
Records fetal heart rate (FHR) in relation to movements.
### **Principle**
**Accelerations = Reassuring indicator of fetal oxygenation and autonomic function.**
### **Procedure**
* Duration: 20 minutes (extend to 40 min if non-reactive)
* Interpretation based on ≥32 weeks criteria.
### **NST Interpretation**
#### **Reactive NST**
* **≥2 accelerations** in 20 min
* Acceleration: **≥15 bpm for ≥15 sec** (≥10 bpm for ≥10 sec if <32 weeks)
**Significance:** Normal fetal oxygenation.
#### **Non-Reactive NST**
* <2 accelerations in 40 minutes
* Could be due to sleep cycle/hypoxia/CNS depression.
👉 **Next step:** BPP or CST.
---
## **4.3 Contraction Stress Test (CST) / Oxytocin Challenge Test**
Evaluates **FHR response to induced uterine contractions** → stresses placenta.
### **Method**
* Use nipple stimulation or dilute oxytocin.
### **Positive CST**
* **Late decelerations** with ≥50% contractions
### **Interpretation**
* **Negative CST:** No late decels → reassuring
* **Positive CST:** Repetitive late decels → **Delivery needed**
* **Equivocal:** Intermittent decels
---
## **4.4 Biophysical Profile (BPP)**


Five parameters (each scored 0 or 2):
1. **NST**
2. **Fetal breathing movements**
3. **Gross body movements**
4. **Fetal tone**
5. **Amniotic fluid volume** (Single deepest pocket ≥2 cm)
### **Scoring**
| Score | Interpretation |
| -------- | -------------------------------- |
| **8–10** | Normal |
| **6** | Equivocal — repeat in 24 hrs |
| **≤4** | Abnormal → **Consider delivery** |
---
## **4.5 Modified BPP**
* **NST + Amniotic Fluid Index (AFI)**
Normal if:
* Reactive NST **AND** AFI >5 cm
---
## **4.6 Doppler Velocimetry**
Essential in **FGR, placental insufficiency, preeclampsia**.
### **Umbilical Artery Doppler**
* **Normal:** High diastolic flow
* **Abnormal findings:**
* **Increased S/D ratio** (placental resistance)
* **Absent end-diastolic flow (AEDF)**
* **Reversed end-diastolic flow (REDF)** → **severe compromise** → urgent delivery
### **Middle Cerebral Artery (MCA) Doppler**
* Low resistance → brain sparing in hypoxia.
* Used in **anemia** (MCA PSV >1.5 MoM).
### **Ductus Venosus Doppler**
* Abnormal A-wave → impending fetal acidemia.
---
# ⭐ **5. Interpretation Summary Table**
| Test | Normal | Abnormal |
| --------------------- | ---------------------- | ---------------------- |
| **Kick Count** | 10 kicks ≤2 hrs | <4/hr or ↓ movements |
| **NST** | Reactive | Non-reactive |
| **CST** | Negative | Positive (late decels) |
| **BPP** | 8–10 | ≤4 |
| **Modified BPP** | Reactive + AFI >5 | Any abnormal |
| **Umb. Art. Doppler** | Forward diastolic flow | AEDF/REDF |
---
# ⭐ **6. Clinical Decision Making**
### If **NST reactive** → Continue routine surveillance
### If **NST non-reactive** → Do BPP or CST
### If **BPP ≤4** → **Deliver**
### If **CST positive** → **Deliver**
### If **Umbilical artery REDF** → **Immediate delivery** (after steroid coverage if possible)
---
# ⭐ **7. Frequency of Testing**
| Condition | Frequency |
| ---------------------- | ------------------ |
| Diabetes, hypertension | Weekly or biweekly |
| FGR | 2–3 times/week |
| Post-term | Daily NST/BPP |
| Oligohydramnios | 2–3 times/week |
---
If you want, I can also generate:
✅ **30 case scenarios with management**
✅ **20–30 MCQs (exam-style)**
✅ **HTML/CSS/JS interactive quiz**
✅ **Printable PDF notes**
Just tell me what you need!



















Comments (3)

Medical Student
This was incredibly helpful for my upcoming exam. Thank you!
Nursing Professional
Great explanation of the ECG changes in hyperkalemia!