Murphy’s Sign in Acute Cholecystitis – Definition, Technique, Diagnosis Clinical Importance
Below is a **complete, concise-but-exhaustive medical reference** on **Murphy’s Sign**, following your preferred “single-place expanded pattern.”
---
# **Murphy’s Sign – Complete Medical Reference**


---
## **1. Definition**
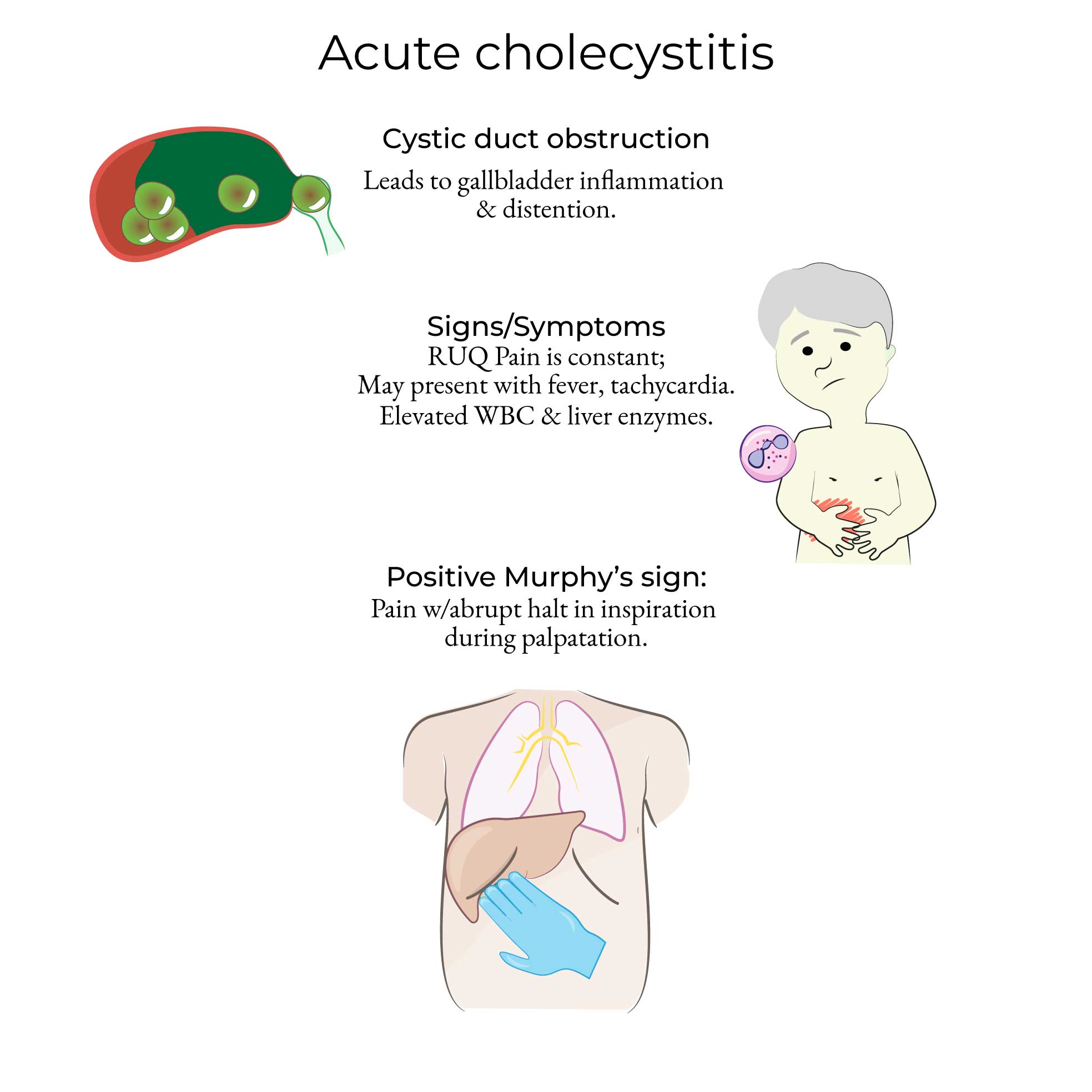
**Murphy’s sign** is a **clinical sign for acute cholecystitis**.
It is **positive** when **deep palpation of the right upper quadrant (RUQ) causes the patient to abruptly stop inspiration due to pain**.
---
## **2. How to Elicit the Sign (Examination Technique)**
1. Ask the patient to **lie supine**.
2. Place your **right hand** below the **right costal margin** at the **mid-clavicular line** (gallbladder location).
3. Ask the patient to **take a deep breath**.
4. A **positive Murphy’s sign**:
* **Sharp pain occurs**, causing the patient to **halt inspiration abruptly**.
* Often accompanied by **facial grimace**.
**Note:** The sign is **absent in elderly** or **diabetic patients** despite severe disease due to neuropathy.
---
## **3. Pathophysiology (Why It Happens)**
* During inspiration, the **diaphragm descends**, pushing the **inflamed gallbladder** downwards.
* When the examiner’s hand is placed at the gallbladder area, the inflamed organ **touches the palpating fingers**, causing **severe pain**, leading to **arrest of inspiration**.
---
## **4. Causes of Positive Murphy’s Sign**
Primary cause:
* **Acute calculous cholecystitis** (most common)
* **Acute acalculous cholecystitis** (critically ill, trauma, burns)
Other rare causes include:
* Severe **cholelithiasis with inflammation**
* **Gallbladder empyema**
* **Pericholecystic abscess**
* **Gallbladder carcinoma** presenting with acute inflammation
---
## **5. Clinical Features Associated with Murphy’s Sign**
* RUQ pain
* Fever
* Nausea/vomiting
* Localized tenderness
* Rebound tenderness may be absent (deep organ)
* Leukocytosis
* Mild jaundice (if obstruction of CBD; “Mirizzi syndrome” possible)
---
## **6. Diagnostic Value**
### **Sensitivity & Specificity**
* **Sensitivity:** 60–90% for acute cholecystitis
* **Specificity:** ~85%
* **More reliable** in **younger** and **non-diabetic** patients
### **Ultrasonographic Murphy’s Sign**
* Pain when the **ultrasound probe presses** over the gallbladder
* **More accurate** than clinical Murphy’s sign
* Key part of **Tokyo Guidelines** diagnostic criteria for cholecystitis
---
## **7. Differential Diagnosis**
Conditions causing RUQ pain but **Murphy’s sign negative** usually:
* **Peptic ulcer disease**
* **Pancreatitis**
* **Renal colic (right)**
* **Hepatitis**
* **Right lower lobe pneumonia**
* **Fitz-Hugh–Curtis syndrome**
* **Biliary colic** (no inflammation → Murphy’s negative)
---
## **8. Investigations When Murphy’s Sign Is Positive**
1. **Ultrasound abdomen**
* Gallbladder wall thickening (>3 mm)
* Pericholecystic fluid
* Gallstones
* Sonographic Murphy’s sign
2. **CBC**
* Leukocytosis
3. **LFTs**
* Elevated ALP, GGT; mild ↑ bilirubin
4. **CRP**
* Elevated in infection
5. **HIDA scan** (if USG inconclusive)
* Non-visualization of gallbladder = cholecystitis
---
## **9. Management (Based on Murphy’s Positive + Clinical/Lab Findings)**
### **1. Initial Stabilization**
* NPO (nil per oral)
* IV fluids
* IV analgesics (Avoid morphine → sphincter of Oddi spasm; preferred: **NSAIDs or tramadol**)
* IV antibiotics (see below)
### **2. Antibiotics**
**Indication:** Suspected acute cholecystitis
**Common regimens:**
* **Ceftriaxone + Metronidazole**
* **Piperacillin–tazobactam** (severe cases)
* **In penicillin allergy:** Ciprofloxacin + Metronidazole
### **3. Definitive Treatment**
**Early laparoscopic cholecystectomy (within 72 hours)** is standard of care.
### **4. For high-risk / critically ill**
* **Percutaneous cholecystostomy**
* Interval cholecystectomy once stabilized
---
## **10. Drug Details (As Per Your Pattern)**
### **🔸 NSAIDs (e.g., Diclofenac, Ketorolac)**
**Indication:** Pain control
**MOA:** COX inhibition → ↓ prostaglandins → analgesia
**Dose:** Diclofenac 50–75 mg IM; Ketorolac 30 mg IV
**Effects:** GI upset, renal injury
**Contraindications:** Renal failure, GI bleed
**Counselling:** Take with food, avoid in dehydration
---
### **🔸 Antibiotics (example: Ceftriaxone)**
**Indication:** Infection in acute cholecystitis
**MOA:** Inhibits bacterial cell wall synthesis
**Dose:** 1–2 g IV daily
**Adverse effects:** Allergy, diarrhea
**Contraindications:** Cephalosporin allergy
**Counselling:** Report rash; complete the course
---
### **🔸 Metronidazole**
**Indication:** Anaerobic coverage
**MOA:** DNA damage in anaerobic bacteria
**Dose:** 500 mg IV q8h
**Adverse:** Metallic taste, disulfiram reaction
**Contraindication:** Alcohol use
**Counselling:** Avoid alcohol for 48–72 hrs
---
## **11. Complications if Murphy’s Sign Indicates Untreated Cholecystitis**
* Empyema
* Gangrene
* Perforation
* Peritonitis
* Sepsis
* Biliary fistula
* Gallstone ileus
---
## **12. Quick Memory Trick**
**“Murphy Stops the Breath.”**
If pain **stops inspiration**, **think cholecystitis**.
---
If you want, I can also give:
✅ **SEO title + description + keywords**
✅ **Case-based MCQs on Murphy’s sign**
✅ **HTML/CSS/JS interactive quiz**
Just tell me!
---
# **Murphy’s Sign – Complete Medical Reference**



---
## **1. Definition**
**Murphy’s sign** is a **clinical sign for acute cholecystitis**.
It is **positive** when **deep palpation of the right upper quadrant (RUQ) causes the patient to abruptly stop inspiration due to pain**.
---
## **2. How to Elicit the Sign (Examination Technique)**
1. Ask the patient to **lie supine**.
2. Place your **right hand** below the **right costal margin** at the **mid-clavicular line** (gallbladder location).
3. Ask the patient to **take a deep breath**.
4. A **positive Murphy’s sign**:
* **Sharp pain occurs**, causing the patient to **halt inspiration abruptly**.
* Often accompanied by **facial grimace**.
**Note:** The sign is **absent in elderly** or **diabetic patients** despite severe disease due to neuropathy.
---
## **3. Pathophysiology (Why It Happens)**
* During inspiration, the **diaphragm descends**, pushing the **inflamed gallbladder** downwards.
* When the examiner’s hand is placed at the gallbladder area, the inflamed organ **touches the palpating fingers**, causing **severe pain**, leading to **arrest of inspiration**.
---
## **4. Causes of Positive Murphy’s Sign**
Primary cause:
* **Acute calculous cholecystitis** (most common)
* **Acute acalculous cholecystitis** (critically ill, trauma, burns)
Other rare causes include:
* Severe **cholelithiasis with inflammation**
* **Gallbladder empyema**
* **Pericholecystic abscess**
* **Gallbladder carcinoma** presenting with acute inflammation
---
## **5. Clinical Features Associated with Murphy’s Sign**
* RUQ pain
* Fever
* Nausea/vomiting
* Localized tenderness
* Rebound tenderness may be absent (deep organ)
* Leukocytosis
* Mild jaundice (if obstruction of CBD; “Mirizzi syndrome” possible)
---
## **6. Diagnostic Value**
### **Sensitivity & Specificity**
* **Sensitivity:** 60–90% for acute cholecystitis
* **Specificity:** ~85%
* **More reliable** in **younger** and **non-diabetic** patients
### **Ultrasonographic Murphy’s Sign**
* Pain when the **ultrasound probe presses** over the gallbladder
* **More accurate** than clinical Murphy’s sign
* Key part of **Tokyo Guidelines** diagnostic criteria for cholecystitis
---
## **7. Differential Diagnosis**
Conditions causing RUQ pain but **Murphy’s sign negative** usually:
* **Peptic ulcer disease**
* **Pancreatitis**
* **Renal colic (right)**
* **Hepatitis**
* **Right lower lobe pneumonia**
* **Fitz-Hugh–Curtis syndrome**
* **Biliary colic** (no inflammation → Murphy’s negative)
---
## **8. Investigations When Murphy’s Sign Is Positive**
1. **Ultrasound abdomen**
* Gallbladder wall thickening (>3 mm)
* Pericholecystic fluid
* Gallstones
* Sonographic Murphy’s sign
2. **CBC**
* Leukocytosis
3. **LFTs**
* Elevated ALP, GGT; mild ↑ bilirubin
4. **CRP**
* Elevated in infection
5. **HIDA scan** (if USG inconclusive)
* Non-visualization of gallbladder = cholecystitis
---
## **9. Management (Based on Murphy’s Positive + Clinical/Lab Findings)**
### **1. Initial Stabilization**
* NPO (nil per oral)
* IV fluids
* IV analgesics (Avoid morphine → sphincter of Oddi spasm; preferred: **NSAIDs or tramadol**)
* IV antibiotics (see below)
### **2. Antibiotics**
**Indication:** Suspected acute cholecystitis
**Common regimens:**
* **Ceftriaxone + Metronidazole**
* **Piperacillin–tazobactam** (severe cases)
* **In penicillin allergy:** Ciprofloxacin + Metronidazole
### **3. Definitive Treatment**
**Early laparoscopic cholecystectomy (within 72 hours)** is standard of care.
### **4. For high-risk / critically ill**
* **Percutaneous cholecystostomy**
* Interval cholecystectomy once stabilized
---
## **10. Drug Details (As Per Your Pattern)**
### **🔸 NSAIDs (e.g., Diclofenac, Ketorolac)**
**Indication:** Pain control
**MOA:** COX inhibition → ↓ prostaglandins → analgesia
**Dose:** Diclofenac 50–75 mg IM; Ketorolac 30 mg IV
**Effects:** GI upset, renal injury
**Contraindications:** Renal failure, GI bleed
**Counselling:** Take with food, avoid in dehydration
---
### **🔸 Antibiotics (example: Ceftriaxone)**
**Indication:** Infection in acute cholecystitis
**MOA:** Inhibits bacterial cell wall synthesis
**Dose:** 1–2 g IV daily
**Adverse effects:** Allergy, diarrhea
**Contraindications:** Cephalosporin allergy
**Counselling:** Report rash; complete the course
---
### **🔸 Metronidazole**
**Indication:** Anaerobic coverage
**MOA:** DNA damage in anaerobic bacteria
**Dose:** 500 mg IV q8h
**Adverse:** Metallic taste, disulfiram reaction
**Contraindication:** Alcohol use
**Counselling:** Avoid alcohol for 48–72 hrs
---
## **11. Complications if Murphy’s Sign Indicates Untreated Cholecystitis**
* Empyema
* Gangrene
* Perforation
* Peritonitis
* Sepsis
* Biliary fistula
* Gallstone ileus
---
## **12. Quick Memory Trick**
**“Murphy Stops the Breath.”**
If pain **stops inspiration**, **think cholecystitis**.
---
If you want, I can also give:
✅ **SEO title + description + keywords**
✅ **Case-based MCQs on Murphy’s sign**
✅ **HTML/CSS/JS interactive quiz**
Just tell me!



















Comments (3)

Medical Student
This was incredibly helpful for my upcoming exam. Thank you!
Nursing Professional
Great explanation of the ECG changes in hyperkalemia!